

Pulmonary arterial hypertension (PAH) is a severe cardiovascular disease characterized by vascular thickening and remodeling, obstruction of blood flow and right heart strain.
Untreated PAH presents as shortness of breath, fatigue, chest pain and tachycardia. If symptoms are left to progress, they can ultimately lead to right heart failure and death (Cassady, 2020; Rosenkranz, 2020). Here, we take a high-level look at two cardiovascular therapies to explore each of their merits, drawbacks and considerations for the future of pharmacological research in the field of PAH.
Sildenafil has long been established as a safe, effective and affordable first-line therapy for PAH patients. As a widely-available oral therapeutic, patients have reported improvements in their exercise capacity and overall quality of life (Benavides-Cordoba et al., 2025; Montani, 2013; Croom & Curran, 2008). However, although traditionally used compounds like sildenafil provide symptomatic relief, fundamental structural disease processes are not reversed by the use of this drug class. Newer therapeutics such as sotatercept have recently gained attention for targeting pathologic signaling and remodeling in PAH patients (Joshi et al., 2023). Although there has been much support for the ability of sotatercept (or its murine analog, RAP-011) to reverse PAH pathology at even greater levels than sildenafil (Joshi et al., 2021), its longer-term safety profile has not yet been established.
Perhaps the most notable distinction between sildenafil and sotatercept is in their mechanisms of action. Sildenafil is a phosphodiesterase-5 (PDE-5) inhibitor, effectively relaxing the smooth muscle in the pulmonary arteries, promoting vasodilation, lowering blood pressure in the lungs, and leading to a reduced cardiac workload (Saggar et al., 2025; Ruopp & Cockrill, 2022; Bhogal et al., 2019). Alternatively, sotatercept is an activin receptor type IIA (ActRIIA) fusion protein, which has been shown to target vascular remodeling at the cellular level, thereby restoring normal signaling, reducing inflammation and preventing excess cellular proliferation in the pulmonary arteries (Joshi et al., 2023; Joshi et al., 2022; Madonna & Ghelardoni, 2025). Therefore, while traditional PAH therapies such as sildenafil have primarily focused on vasodilation that offers symptomatic relief, novel therapies such as sotatercept are now targeting the fundamental underlying disease processes.
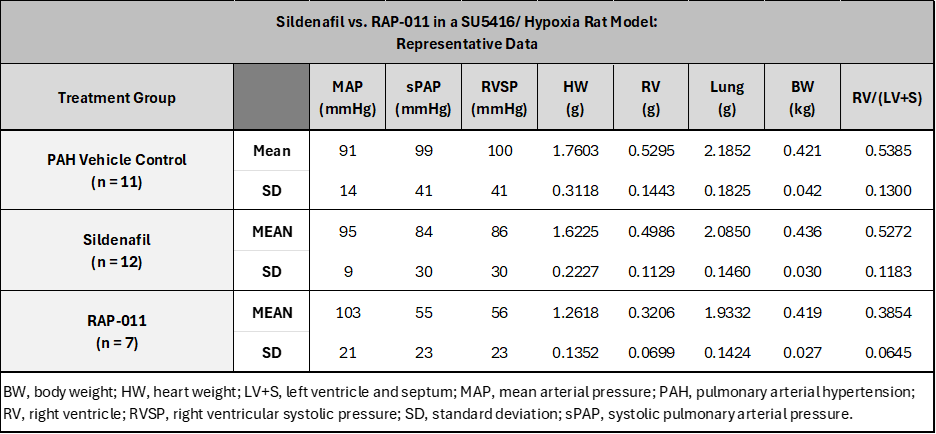
Sildenafil has long been used as a safe, reliable and efficacious therapeutic in the treatment of PAH. However, within a multitude of preclinical studies, sotatercept has recently demonstrated superior level of efficacy as compared to sildenafil (Kopeć et al., 2025; Afra et al., 2024; Pitre et al., 2024; Joshi et al., 2021). At CorDynamics, our team has firsthand experience with each of these compounds and can attest to both of their reliable efficacy in our disease models. In a representative PAH study utilizing a SU5416/ hypoxia rat model, we saw that even when sildenafil did not notably ameliorate the development of PAH as compared to our PAH vehicle control group, animals treated with RAP-011 presented with notable decreases in sPAP (-44%), RVSP (-44%) and Fulton’s Index (-28%); see Text Table 1 for this representative dataset.
Text Table 1. Sildenafil vs. RAP-011 in a SU5416/ Hypoxia Rat Model: Representative Data
This comparison of sildenafil and RAP-011 as therapeutic agents for PAH demonstrates that both compounds have definitive strengths and weaknesses, distinct mechanisms of action, and various levels of efficacy; see Text Table 2 for a high-level comparison of sildenafil and sotatercept. Overall, while sildenafil has a long-established history of both safety and efficacy, sotatercept has made a strong name for itself as a promising “up-and-comer” that may just give sildenafil a run for its money.
Text Table 2. Sildenafil vs. Sotatercept: A High-Level Comparison

Works Cited
- Afra, L. G., Mousavi, A., Mirzaei, M., Rahimi, Y., Khosravi, F., & Rahmanian, M. (2024). Efficacy and Safety of Sotatercept in Pulmonary Arterial Hypertension: A Systematic Review. International Cardiovascular Research Journal, 18(1).
- Benavides-Cordoba, V., Palacios, M., & Vonk-Noordegraaf, A. (2025). Historical milestones and future horizons: exploring the diagnosis and treatment evolution of the pulmonary arterial hypertension in adults. Expert Opinion on Pharmacotherapy, 26(6), 743-753.
- Bhogal, S., Khraisha, O., Al Madani, M., Treece, J., Baumrucker, S. J., & Paul, T. K. (2019). Sildenafil for pulmonary arterial hypertension. American journal of therapeutics, 26(4), e520-e526.
- Cassady, S. J., & Ramani, G. V. (2020). Right heart failure in pulmonary hypertension. Cardiology clinics, 38(2), 243-255.
- Croom, K. F., & Curran, M. P. (2008). Sildenafil: a review of its use in pulmonary arterial hypertension. Drugs, 68(3), 383-397.
- Joshi, S. R., Liu, J., Andre, P., Kumar, R., & Li, G. (2021). Sotatercept Analog RAP-011 is More Effective Than Sildenafil in Improving Pulmonary Hypertension and Reducing Right Ventricular Hypertrophy in a ZSF1 Rat Model of Heart Failure With Preserved Ejection Fraction. Circulation, 144(Suppl_1), A12203-A12203.
- Joshi, S. R., Atabay, E. K., Liu, J., Ding, Y., Briscoe, S. D., Alexander, M. J., … & Li, G. (2023). Sotatercept analog improves cardiopulmonary remodeling and pulmonary hypertension in experimental left heart failure. Frontiers in Cardiovascular Medicine, 10, 1064290.
- Joshi, S. R., Liu, J., Bloom, T., Karaca Atabay, E., Kuo, T. H., Lee, M., … & Li, G. (2022). Sotatercept analog suppresses inflammation to reverse experimental pulmonary arterial hypertension. Scientific reports, 12(1), 7803.
- Kopeć, G., Skride, A., Ereminiene, E., Simkova, I., Enache, R., Samarzija, M., … & Jansa, P. (2025). Emerging therapies and new directions in the treatment of pulmonary arterial hypertension. Polish Heart Journal (Kardiologia Polska), 83(1), 18-26.
- Madonna, R., & Ghelardoni, S. (2025). Sotatercept in pulmonary hypertension and beyond. European Journal of Clinical Investigation, 55(5), e14386.
- Montani, D., Günther, S., Dorfmüller, P., Perros, F., Girerd, B., Garcia, G., … & Sitbon, O. (2013). Pulmonary arterial hypertension. Orphanet journal of rare diseases, 8(1), 97.
- Pitre, T., Desai, K., Mah, J., Zeraatkar, D., & Humbert, M. (2024). Comparative effectiveness of sotatercept and approved add-on pulmonary arterial hypertension therapies: a systematic review and network meta-analysis. Annals of the American Thoracic Society, 21(8), 1194-1203.
- Rosenkranz, S., Howard, L. S., Gomberg-Maitland, M., & Hoeper, M. M. (2020). Systemic consequences of pulmonary hypertension and right-sided heart failure. Circulation, 141(8), 678-693.
- Ruopp, N. F., & Cockrill, B. A. (2022). Diagnosis and treatment of pulmonary arterial hypertension: a review. Jama, 327(14), 1379-1391.
- Saggar, R., Rahhali, N., Senatore, A., Sandros, M., Lopez, D., Gomez Rendon, G., … & Sahay, S. (2025). A Systematic Literature Review Exploring the Efficacy and Safety of Tadalafil and Sildenafil in Pulmonary Arterial Hypertension. Pulmonary Circulation, 15(4), e70212.

